During the pandemic, practices have had to navigate an ever-changing list of infection control guidelines and protocols.
While the coronavirus disease 2019 pandemic rages unfettered, health care professionals must continue to treat patients. The Centers for Disease Control and Prevention (CDC) has recommended limiting elective procedures to decrease the risk of spreading COVID-19, they also advise implementing certain protocols to protect health care professionals and patients.
In a news release from the American Dental Association (ADA) published May 29, ADA President Chad Gehani, DDS, said, “Oral health is an important part of overall health. Resuming regular dental visits are important because treatment, as well as prevention of dental disease, helps keep people healthy. [Guidelines] from the ADA and the CDC give dental professionals the information they need to practice as safely as possible.”
Reducing Facility Risk
Scientists believe it’s possible for a person to contract COVID-19 by touching an infected surface and then touching their face. However, the virus is thought to spread mainly from person to person, particularly when people are within 6 feet of each other and an infected person coughs, sneezes, or talks, producing droplets that can be inhaled by others nearby. Not everyone who is infected shows symptoms of COVID-19, so a person who is infected could unknowingly spread the virus.
The dental chair is an excellent location for the virus to spread if proper precautions aren’t taken. The CDC has published recommendations for dental health care personnel (DHCP) who expand care to non-emergency patients.
To help prevent the spread of COVID-19, the CDC earlier had recommended reducing facility risk by canceling elective procedures and offering telemedicine when possible. Other key recommendations include limiting points of entry, implementing source control for everyone who enters the facility, and screening for symptoms. However, because infected patients could be asymptomatic, it is necessary to act as if all patients and providers potentially are carriers.
To protect health care personnel, the CDC recommends emphasizing hand hygiene and limiting the number of staff providing care.
As dental practices see patients during the ongoing pandemic, staff will need to rely on
COVID-19 Resources for Dental Professionals
American Dental Association COVID-19 Practice Resources: bit.ly/ADAPracticeResources. The ADA offers a slew of COVID-19 related resources for practices that are updated regularly, including:
Diagnostic testing options
ADA Foundation Assistance Program
Steps to follow when a patient tests positive for COVID-19
Contact tracing and HIPAA disclosures
Employees and staff issues
Cybersecurity
Patient communications
ADA State Mandates and Regulations: bit.ly/ADAStateRegs
An interactive map provides the latest information from state-to-state, including the current number of cases, mandates from the state government, and recommendations from state dental boards
ADA Mental Health Resources: bit.ly/ADAMentalHealth
Features online, on-demand courses covering stress, anxiety, and staying health during the pandemic
Personal help hotline information
Mental health resources from the National Alliance on Mental Health and the American Foundation for Suicide Prevention, among others
Tips for staying well during isolation
Centers for Disease Control and Prevention Guidance for Dental Settings: bit.ly/CDCDentalSettings. The CDC’s COVID protocol, last updated June 17, offers practices guidance covering:
Patient management
Facility considerations
Equipment considerations
Administrative controls and work practices
Hygiene
Personal protective equipment (PPE)
PPE supply strategies
Environmental infection control
Sterilization and disinfection of patient-care items
CDC Infection Prevention and Control Recommendations for Healthcare Personnel: bit.ly/CDCIC
Telehealth and triage protocols
Screening for signs and symptoms of COVID-19
Implementing universal source control measures
Encouraging physical distancing
Performing targeted SARS-CoV-2 testing of patients without symptoms
Optimizing indoor air quality
Creating a rapid response to SARS-CoV-2 exposure
personal protective equipment (PPE). However, the CDC states that PPE is the least effective control, as it depends on proper fit and correct, consistent use. Also note ongoing and intermittent shortages of PPE in the U.S., including N95 respirators, facemasks, eye protection, gowns, and gloves. Each facility is responsible for finding alternatives to protect their providers when recommended PPE is unavailable.
Alternatives to N95 masks include a respirator that offers a higher level of protection, such as other disposable filtering facepiece respirators, powered air-purifying respirators, or elastomeric respirators.1 N95 masks can be used for extended use (keeping the mask on for encounters with several patients) and limited reuse (using the same respirator for multiple patient encounters, but removing it between encounters), but the CDC advises the respirators be discarded following aerosol-generating procedures (AGP). The advised practice in the dental office is to don a new N95 respirator for each patient who is assumed to be non-contagious, as well as to use eye protection (goggles or full-face shield), gloves, and gowns.
The number of staff present during AGPs should be limited, and room surfaces should be cleaned and disinfected promptly. The Environmental Protection Agency’s “List N: Disinfectants for Use Against SARS-CoV-2 (COVID-19),” lists disinfectants currently available as well as instructions for using them.2 For more information about cleaning rooms and PPE, refer to the CDC’s “Clinical Questions about COVID-19: Questions and Answers.”3
The CDC offers several recommendations for health care facilities to limit the risk of exposure and transmission of COVID-19. It’s important to remember these practices are recommended for all patients, not just those who are or may be infected.
CDC recommended infection prevention and control practices for routine activities during the pandemic include:
Implement telehealth and triage protocols, and postpone any non-urgent visits. Patients should reschedule non-emergency appointments if they have symptoms of COVID-19 on the day of the appointment.
Screen everyone who enters the facility for signs and symptoms of COVID-19. Make sure patients are wearing face coverings or face masks and take their temperatures. If a patient’s temperature is below 100.4° F and they are asymptomatic, dental care may be provided. Limit points of entry and post visual aids about wearing face masks and performing hand hygiene. The practice should also provide hand sanitizer, tissues, and no-touch trash cans.
Implement universal source control measures, such as wearing cloth face coverings or face masks that cover a person’s nose and mouth. The only people who should not wear masks are children under 2 and anyone who has trouble breathing or is unable to remove the mask without assistance. Patients should have their mouths and noses covered whenever they are not in the dental chair.
Encourage physical distancing of 6 feet.
Implement universal use of PPE. This includes a face shield or goggles, a face mask, gloves, and an isolation gown.
Optimize engineering controls and indoor air quality. Use physical barriers and vacuum shrouds for aerosol-generating surgical procedures, as well as optimizing air-handling systems or adding a portable HEPA filtration unit where permanent air-handling systems are not an option.
Create a process to respond to exposures. Request that patients inform the practice if they develop symptoms or are diagnosed with COVID-19 within 2 days following their dental appointment. The practice should have a process for notifying the local health department of any suspected or confirmed cases of infection and performing contact tracing.
Staff should perform hand hygiene before and after all patient contact, after contact with potentially infectious material, and before donning and after removing PPE.
Hands should be washed with soap and water for at least 20 seconds and sanitized with alcohol-based hand sanitizer containing 60% to 95% alcohol.
All PPE should be in accordance with OSHA PPE standards4, and all staff should be trained on when to use PPE, what PPE is necessary, how to put on and take off PPE to prevent self-contamination, how to dispose of or disinfect and maintain PPE, and the limitations of PPE.
Waiting Rooms
The CDC advises that chairs in the waiting room be placed at least 6 feet apart.5 Toys, magazines, and other frequently touched objects that can’t be regularly cleaned or disinfected should be removed from the waiting area. The number of patients in the waiting room should be kept to a minimum; avoid overlapping dental appointments.
Equipment
Because practices are reopening after a period of closure, manufacturers’ instructions for use should be reviewed for the following: Dental unit waterlines, autoclaves and instrument cleaning equipment, air compressors, vacuum and suction lines, radiography equipment, high-tech equipment, amalgam separators, and other dental equipment. The CDC has published an article titled “Guidance for Reopening Buildings After Prolonged Shutdown or Reduced Operation” for further reference.6
Administrative Controls
Health care personnel should limit clinical care to 1 patient at a time. Operatories should be set up so that only clean and sterile supplies needed for the procedure are readily accessible. Everything else should be in covered storage. Aerosol-generating procedures should be avoided in favor of minimally invasive and atraumatic restorative techniques that use hand instruments instead of ultrasonic scalers.
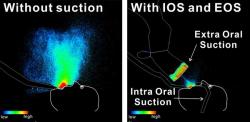
If AGPs can’t be avoided, the CDC recommends the use of 4-handed dentistry, high volume evacuation suction, and dental dams. They also recommend preprocedural mouth rinses such as chlorhexidine gluconate.
Because scientists are continuing to learn more about this virus, recommendations are constantly changing. It is strongly advised that you regularly consult the CDC, OSHA, and your state dental boards directly for any new information on providing treatment during this pandemic.
To ensure that everyone in the practice is on the same page, consult the ADA and Organization for Safety, Asepsis and Prevention (OSAP) webinar, “COVID-19 Response—CDC Guidance for Dental Settings,”7 which was recorded May 28 and is available on the ADA website for on-demand viewing, along with other webinars. Attendees can earn 1 continuing education credit from this course.
OSAP and DentaQuest have put together a comprehensive guide outlining the best practices for infection control during the pandemic,8 which includes checklists about preparing the clinic for patient appointments and delivering safe patient care.
Because all of the resources pertaining to providing care during the COVID-19 pandemic are constantly being updated, consult the organizations on a daily basis, particularly the CDC’s Guidance for Dental Settings page, which includes key points and summaries of recent changes at the top of the page.
References
1. Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic. Centers for Disease Control and Prevention.Updated July 15, 2020. Accessed June 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html
2. List N: Disinfectants for Use Against SARS-CoV-2 (COVID-19). United States Environmental Protection Agency. Updated July 9, 2020. Accessed June 2020. https://www.epa.gov/pesticide-registration/list-n-disinfectants-use-against-sars-cov-2-covid-19
3. Clinical Questions about COVID-19: Questions and Answers. Centers for Disease Control and Prevention. Updated July 7, 2020. Accessed June 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-faq.html
4. Regulations (Standards - 29 CFR). Occupational Safety and Health Administration. Accessed June 2020. https://www.osha.gov/laws-regs/regulations/standardnumber/1910
5. Guidance for Dental Settings: Interim Infection Prevention and Control Guidance for Dental Settings During the COVID-19 Response.” Centers for Disease Control and Prevention. Updated June 17, 2020. Accessed June 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.html
6. Guidance for Reopening Buildings After Prolonged Shutdown or Reduced Operation. Centers for Disease Control and Prevention. https://www.cdc.gov/coronavirus/2019-ncov/php/building-water-system.html
7. COVID-19 Response — CDC Guidance for Dental Settings (Recorded Webinar). American Dental Association. Accessed June 2020. https://ebusiness.ada.org/Education/viewcourse.aspx?ID=436
8. OSAP/DQP Best Practices for Infection Control in Dental Clinics During the COVID-19 Pandemic. OSAP and DentaQuest. Updated June 19, 2020. Accessed June 2020. https://cdn.ymaws.com/www.osap.org/resource/resmgr/dentaquest/INC-1353_Best_Practices_for_.pdf

 Download Issue: Dental Products Report August 2020
Download Issue: Dental Products Report August 2020